
| Home > CF Guidelines > Chest Problems > Viruses & Immunisation |
|
CF Guidelines - Viruses & Immunisation |
||||||||
| Immunisation for people with CF: | ||||||||
| We recommend that all routine childhood vaccinations are given at the usual times and should be arranged by the general practitioner. BCG should be given to appropriate high risk individuals. Influenza immunisation is advised for all children over 6 months, again arranged by the GP. It is useful to remind families and GPs in early autumn with vaccines usually available from October. All children under 12 years old if receiving the vaccine for the first time, a 2nd dose is repeated 4 - 6 weeks later - otherwise it is a single injection annually. | ||||||||
| Dose for each vaccination is determined by age: | ||||||||
- |
6 - 35 months 0.25ml | |||||||
- |
> 35 months 0.5 ml | |||||||
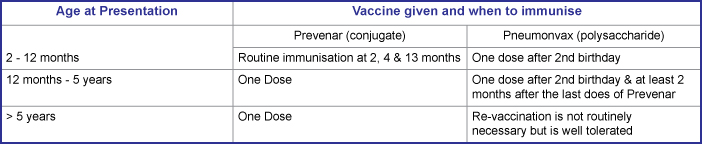
| The vaccine is inactivated (killed) and is given by deep s/c or IM injection in the deltoid (older children) or thigh (infants and young children). Several products are licensed (see British National Formulary) and are interchangeable. History of egg anaphylaxis is a contraindication. Pneumococcal immunisation is now recommended for all children as part of the primary immunisation programme. Children under 2 years produce a poor response to polysaccharide vaccines (e.g. Pneumovax) so the newer conjugate vaccine (Prevenar) is used in this age group. | ||||||||
 |
||||||||
| Chickenpox: | ||||||||
| Chickenpox can cause a pneumonitis and an associated infective exacerbation in CF lungs. Patients on high dose oral steroids or who are immunosuppressed are particularly at risk. This may result in irreversible loss of lung function unless treatment is commenced promptly. | ||||||||
| Patients who are not on oral steroids/immunocompromised: | ||||||||
- |
If early into the course of chickenpox and the patient is unwell give IV acyclovir for 7 - 10 days + IV antibiotics. | |||||||
| Patients who are (or have been) taking oral steroids/immunocompromised: | ||||||||
- |
As above. If they have not had chicken pox previously and are exposed to chicken pox, they should receive Varicella-Zoster Immunoglobulin (VZIG) if they are currently taking oral steroids, or in the last 3 months have had the equivalent of 2mg/kg/day prednisolone for 1 week, or the equivalent of 1mg/kg/day prednisolone for 4 weeks. A second dose of VZIG should be given if further exposure occurs more than 3 weeks after the first dose. | |||||||
| Varicella-susceptible patients on oral steroids that have come into contact with chicken pox or shingles should be reviewed. If a rash develops treat with iv acyclovir. VZIG is given by deep IM injection. | ||||||||
- |
< 5 yrs 250mg. | |||||||
- |
6 - 10 yrs 500mg. | |||||||
- |
11 - 14 yrs 750mg. | |||||||
- |
over 15 yrs 1g. | |||||||
| If chicken pox still develops in these children, IV acyclovir is indicated. | ||||||||
| Dowloadable PDF File - PDF File | ||||||||
Document approved - 2011 |
||||||||
Document due for review - December 2013 |
||||||||
| Acknowledgements: The Peninsula CF team acknowledges the use of guidelines produced by The CF Trust, Manchester, Papworth, Leeds and Brompton CF teams during development of these local Peninsula protocols and guidelines. | ||||||||
| Disclaimer: While efforts have been made to ensure that all the information published on this web site is correct, the authors take no responsibility for the accuracy of information, or for harm arising as a consequence of errors contained within this web site. If you have concerns regarding treatment, drugs or doses then consult your local CF consultant. |
©2009 - 2013 All rights reserved. Peninsula Cystic Fibrosis Network |